- 4192 Devonwood Way, Ashburn, Virginia, 20148
- Helpline: +1 (703) 665-3747
Friedreich’s Ataxia with Hypertrophic Cardiomyopathy and Cardiac Tamponade – A Rare Occurrence
- Home
- Back to Journal
- Article Details
Abstract
Friedreich’s ataxia is the most common inherited spinocerebellar ataxia. Almost all the patients with neurological symptoms have cardiac manifestations, the most common being Hypertrophic Cardiomyopathy (HCM), usually manifesting as diffuse symmetric hypertrophy and rarely as asymmetric hypertrophy. The presence of pericardial effusion along with tamponade in association with HCM is rare and therefore being reported.
Keywords: Friedreich’s ataxia, Hypertrophic cardiomyopathy, pericardial effusion, cardiac tamponade
Introduction
Friedreich’s ataxia is the prototype for the inherited spinocerebellar ataxia. The individual is chair bound by second decade. The cardiac manifestations are seen in almost all cases, the most common being hypertrophic cardiomyopathy. Though mild effusions can be seen in some cases, patient presenting with tamponade is rare. We report such case along with review of the literature.
Case Details
A 10-year-old male child was referred to the cardiology department with complaints of swelling of lower limbs, abdominal distention, and shortness of breath. Swelling of lower limbs was noticed by mother, progressed to whole lower limbs and abdominal distention. Shortness of breath was of sudden onset. On the evaluation of history, it was revealed that he was born out of consanguineous marriage, second in birth order (Figure 1B). The delivery was normal with no complications. He had normal milestones and was immunized to date appropriately for his age. He was diagnosed as having Friedreich’s ataxia, after admission with complaints of frequent buckling and difficulty in walking with deformity of both lower limbs noticed at the age of 5 years.
On evaluation, the child was conscious, tachypneic, with a pulse rate of 130 per min, His blood pressure was recorded 70/50 mmHg over the right upper arm. Physical examination revealed abnormal facies with pouting lips, protruding tongue, scoliosis, bilateral pes cavus (Figure 1C), Spina Bifida occulta. The systemic examination of the cardiovascular system revealed distant heart sounds and the lungs were clear on auscultation.
The Electrocardiogram (ECG) showed sinus tachycardia with a rate of 120 per min, an axis of -150°, and no significant ST-T changes, Left Ventricular Hypertrophy (LVH) by voltage criteria (Figure 1A). The chest x-ray showed cardiomegaly with an LV type of apex and clear lung fields and scoliosis of the thoracic spine (Figure 1D).
The echocardiography showed moderate pericardial effusion with a maximum diameter of 1.6 cm (Figure 2A). There was subtle right atrial and right ventricle collapse in early diastole in favor of cardiac tamponade. The asymmetrical thickness of the walls of the left ventricle was noticed.
An emergency pericardiocentesis was done for the cardiac tamponade. Approximately, 500 ml of clear, straw-colored fluid was drained which was transudate on analysis. The adenosine deaminase level was (ADA) 16U/l and the sugar was 60 mg/dl. The infective pathology was ruled with negative cultures. There was symptomatic and clinical improvement in the patient’s condition after the procedure.
His biochemical profile showed hemoglobin of 12.6 gm per deciliter, the white blood cell count of 6,800cell/mm3 with neutrophils of 65%, lymphocytes of 30%, monocytes of 01%, and eosinophils of 3%. The erythrocyte sedimentation rate was 10 mm 1st hour. Repeat ECG showed no electrical alternans (Figure 2B). The echocardiographic examination revealed normal left ventricular function (Figure 2C). There was increased relative wall thickness, asymmetric hypertrophy of LV, and increased LV mass of 158 gms. The LV mass when indexed to height 2.7 was 99g/m which is severely abnormal increased LV mass for his age [1] (Figure 2D). There was no subsequent fluid accumulation.
The patient had a staggering gait when ambulated. The genetic analysis was not done because of financial constraints. The diagnosis was confirmed based on criteria as per Harding et al. [2] of the skeletal (Figure 3). The patient was discharged in a stable condition.
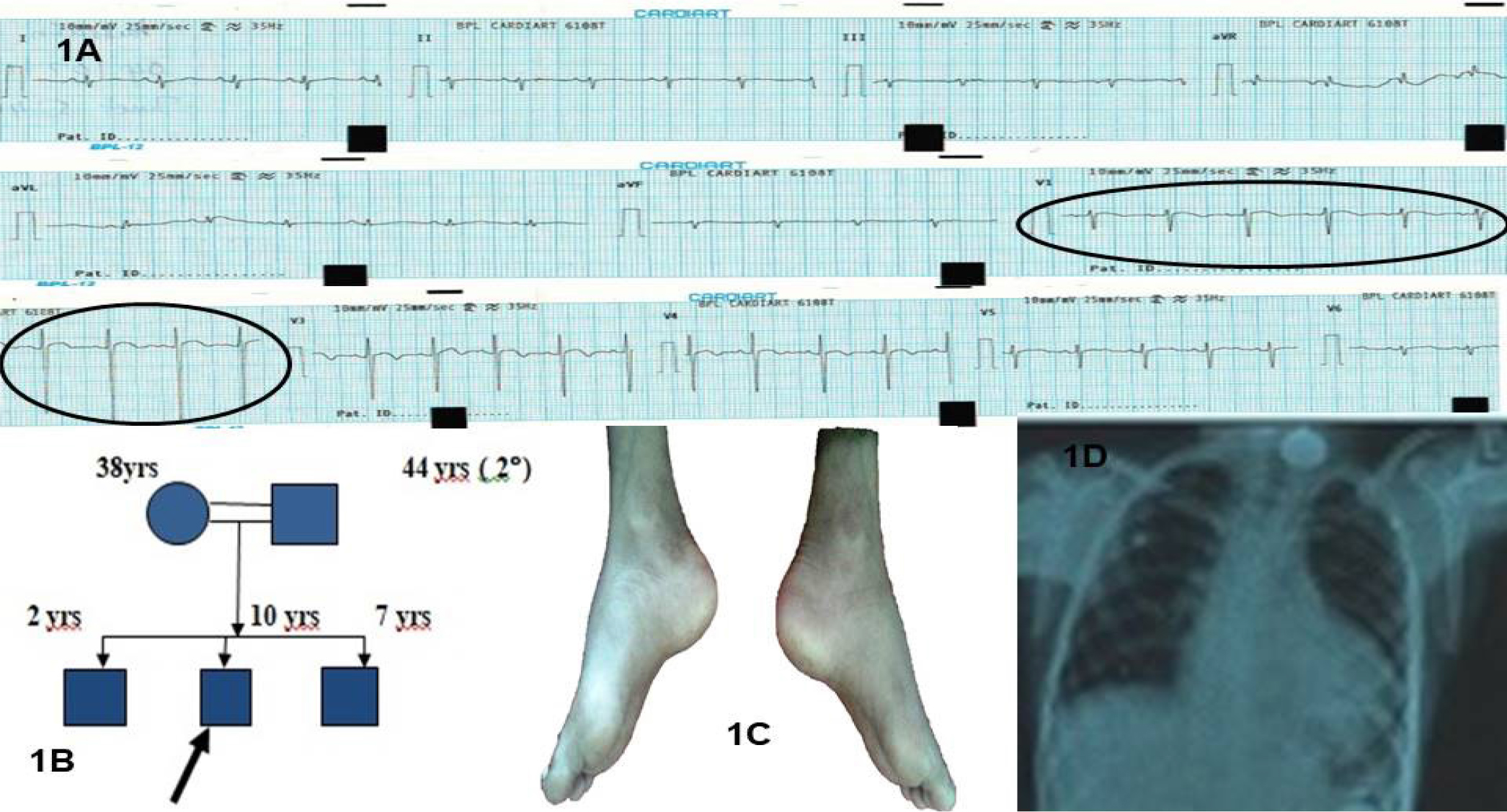
Figure 1: A) Admission electrocardiogram showing electrical alternans evident in Lead V1 and V2. 1B) Pedigree chart of the case. C) Bilateral pes cavus D) Chest x-ray showing moderate cardiomegaly with left ventricular type of apex. There is scoliosis with convexity to the left of the thoracic spine.
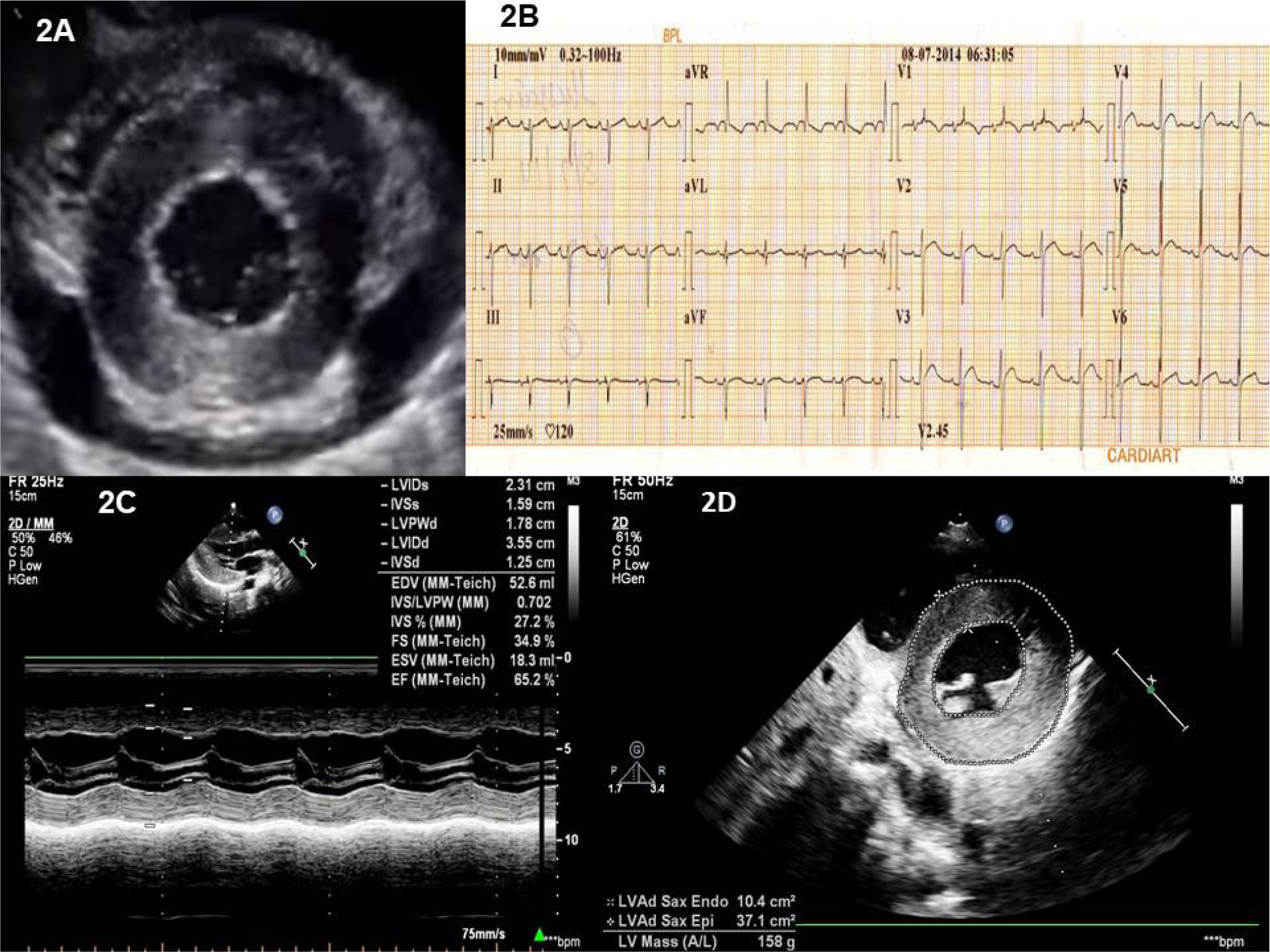
Figure 2: A) Echocardiographic image of the parasternal short axis of the left ventricle at the mid-ventricular level showing moderate circumferential pericardial effusion. Concentric left ventricular hypertrophy is also evident. The pericardium is normal. B) Electrocardiogram after pericardiocentesis showing the absence of electrical alternans. There is biventricular hypertrophy by voltage. There is biatrial enlargement and t wave inversion in lead V1. C) The M mode of the left ventricle just below the mitral leaflets showing normal left ventricular function. The relative wall thickness is 1.00. 2D). LV mass calculation by area length method - a value of 158 gm, when indexed to height 2.7 was 99 (indicating severe abnormal increased LV mass) [1].
Discussion
Friedreich’s ataxia, the autosomal recessive spinocerebellar ataxia is the most common form of inherited ataxia. [3] The disease has a predilection for the involvement of lower more than the upper extremities. The neurological feature is progressive with worsening staggering gait, and frequent falls. Less common presenting features are progressive scoliosis, bilateral foot deformity, nystagmus, or cardiomyopathy.
Cardiac involvement occurs in almost all cases with neurological involvement. The presence of cardiomegaly, symmetric hypertrophy, and conduction defects are commonly reported. Asymmetric hypertrophy is less commonly observed. Our case has cardiomegaly and asymmetric hypertrophy of the left ventricle [4, 5].
The trinucleotide repeat sequence (GAA) in the intron of mutant gene frataxin leads to functional deficiency of aconitase, a mitochondrial enzyme involved in iron homeostasis, subjecting the cell to oxidative stress secondary to iron overload. The left ventricular hypertrophy on electrocardiograms might be absent despite the echocardiographic evidence. Widespread T wave inversions are common. An important differentiating point from the usual genetic HCM is arrhythmias are not common in HCM of Friedreich’s ataxia. The hypertrophy of the myocardium in Friedreich’s ataxia is due to hypertrophy of the mitochondria. There will be no myocardial fiber disarray explaining the absence of ventricular arrhythmias compared to the usual HCM [3].
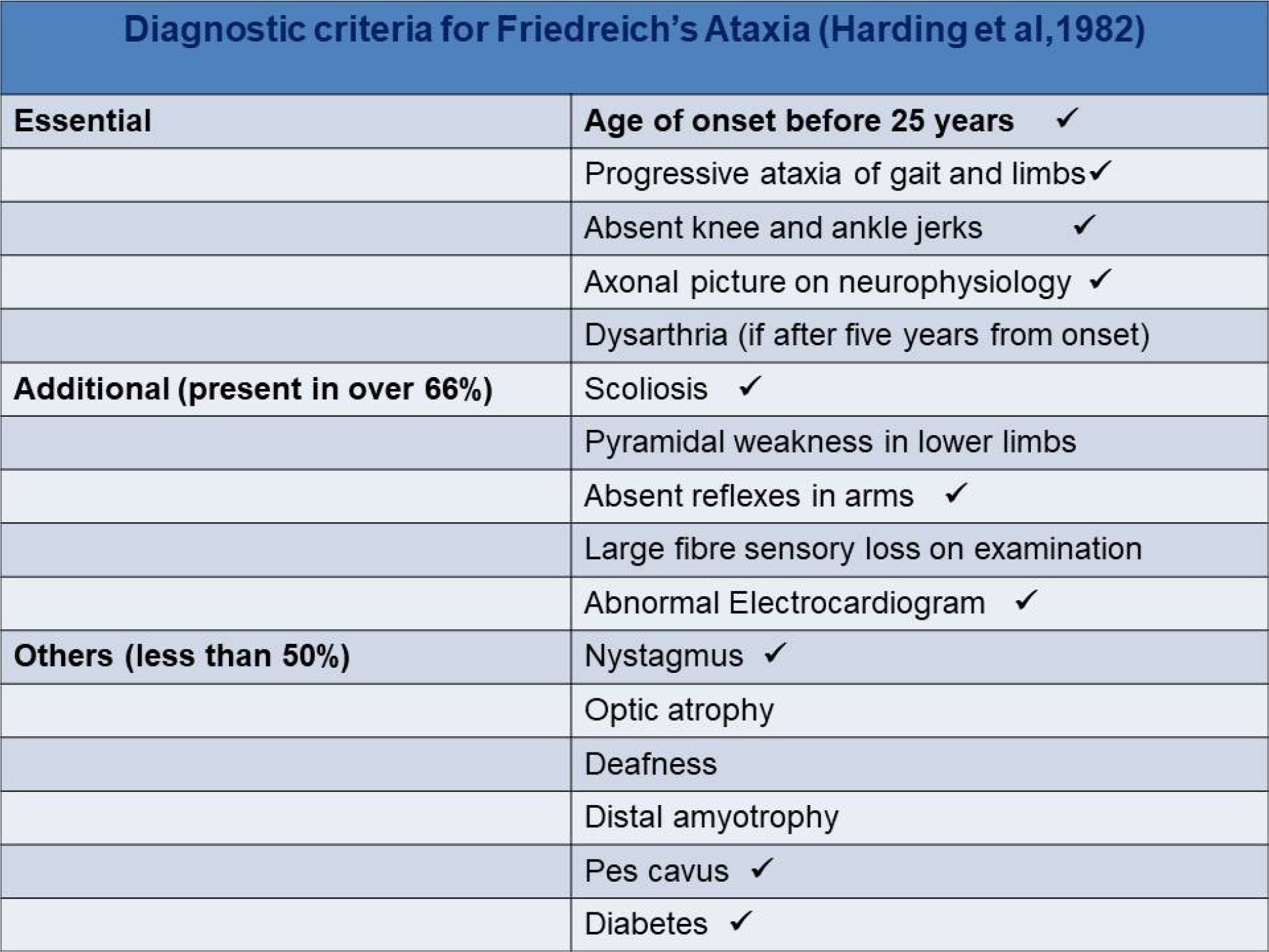
Figure 3: Diagnostic criteria for Friedreich’s ataxia by Harding et al [2].
Tick marks indicate the features present in the case.
A high incidence of diabetes mellitus (20%) is found and is associated with insulin resistance, pancreatic β cell dysfunction. Musculoskeletal deformities are common and include pes cavus, pes equinovarus, and scoliosis [3].
The diagnosis of Friedreich’s ataxia is by clinical (essential, additional, and supportive) along with confirmatory diagnosis by genetic analysis [2]. The more the number of GAA repeats, the earlier the onset of disease, and the worse is the prognosis [2].
The pericardial effusion occurring in Friedreich’s ataxia is a rare entity. A few cases have been reported in patients with hypertrophic cardiomyopathy and early reports on Friedreich’s Ataxia [4–7]. This is the first case of the occurrence of cardiac tamponade in a patient with Friedreich’s ataxia to the best of our knowledge.
The pericardial effusion can be related to the disease itself or can be acquired [5], the most common cause was acute rheumatic fever. The usual echocardiographic features of cardiac tamponade in a patient with severe left ventricular hypertrophy are not evident as the ventricular interdependence with respiration is reduced due to relatively fixed rates of left ventricular filling. There can be only hypotension without pulsus paradoxus clinically but a significant pericardial effusion on echocardiogram as was in our case [8].
Idebenone, a free radical scavenger, decreases the left ventricular hypertrophy and mass in Friedreich’s ataxia patients. Patients with a greater degree of hypertrophy respond best to the drug though it improves neither systolic function nor the neurological outcomes.[1] The most common cause of death is a cardiac failure [9].
Learning Objectives
The occurrence of pericardial effusion in a patient with hypertrophic cardiomyopathy is rare.
The usual features of cardiac tamponade i.e., pulsus paradoxus and respiratory variation indicating ventricular interdependence can be absent in patients with severe left ventricular hypertrophy secondary to fixed filling velocities. Hence, high suspicion of the cardiac tamponade is needed whenever there is ambiguity in a patient with hypertrophic cardiomyopathy and pericardial effusion.
Conclusion
Friedreich’s ataxia with hypertrophic cardiomyopathy is common. Asymmetrical hypertrophy of left ventricle along with cardiac tamponade at presentation is rare. High index of suspicion for tamponade is needed in a case of HCM with pericardial effusion.
Praveen Nagula and K Anjani Kiranmayi are equally contributed
References
- Khoury, Philip R et al (2009) Age-specific reference intervals for indexed left ventricular mass in children. J Am Soc Echocardiogr 22: 709–714. [View]
- Harding AE (1981) Friedreich’s ataxia; a clinical and genetic study of 90 families with an analysis of early diagnostic criteria and intrafamilial clustering of clinical features. Brain 104: 589–620. [View]
- Samuel H, Boyer IV, Arthur WC, Victor AM (1962) Cardiac Aspects of Friedreich’s Ataxia. Circulation 25: 493–505. [View]
- Ellwood WW (1984) Friedreich’s Ataxia with unusual heart complications. Calif Med 68: 296–8. [View]
- Nadas AS, Alimurung MM, Sieracki LA (1951) Cardiac manifestations of Friedreich’s ataxia. N Engl J Med 244: 239–44. [View]
- Nichols L, Koelmeyer H (2019) Hypertrophic cardiomyopathy masked by pericarditis. Autops Case Rep 9: e20191113. [View]
- Kim YM, Kim G, Ko H, Yoo HW, Lee HD (2018) Treatable massive pericardial effusion and hypertrophic cardiomyopathy in an infant with a novel homozygous ACADVL mutation: A case report. Medicine 97: e10813. [View]
- William F. Armstrong MD, Thomas Ryan MD (2018) Pericardial diseases (10th chapter). Feigenbaum’s Echocardiography (7thedn). Wolter Kluwer India Pvt.Ltd Pg No: 253. [View]
- Kipps A, Alexander M, Colan SD, Gauvreau K, Smoot L, Crawford L et al. (2009) The longitudinal course of cardiomyopathy in Friedreich’s Ataxia during childhood. Pediatric Cardiol 30: 306–10.