- 4192 Devonwood Way, Ashburn, Virginia, 20148
- Helpline: +1 (703) 665-3747
Quality of Chest Compression Performed by Healthcare Operators: Results from a Prospective Cohort Study on Manikin
- Home
- Back to Journal
- Article Details
Abstract
The high quality and uninterrupted chest compression is the cornerstone of cardiopulmonary resuscitation. Few previous studies reported the quality of this manoeuvre when it was performed by healthcare operators during an in-hospital cardiopulmonary resuscitation. Aims of our study were to show the quality of chest compression when practised by healthcare operators and to search variables related to better quality. Finally, we tried to correlate self-confidence with this manoeuvre and its real effectiveness.
METHODS: In our prospective cohort study a group of healthcare operators performed a two-minute chest compression cycle using a high fidelity manikin recording the compression score. This value summarized the quality of the whole cycle of cardiopulmonary resuscitation with a ratio taking into account adequate chest compressions over their total number. We considered as adequate a compression score ≥ 75%. Collected data were: age, weight, height, Body Mass Index (BMI), gender, smoke habit, hand applied on the thorax, healthcare role, working area, previous real life resuscitation experience, physical limitations and quality perceived by each operator.
RESULTS: 60 healthcare operators were enrolled. Mean compression score: 70±19%. In only 48% of subjects the quality recorded was adequate. Among variables, previous real experience was related to better quality performance (75±19% vs 65±19%, p 0.04). In nearly 50% of operators who considered their test as adequate we recorded a low quality chest compression.
CONCLUSIONS: quality of chest compression was inadequate in nearly half of the cases even when performed by healthcare professionals. In our study only previous real-life resuscitation experience is related to better performance. Finally, we confirmed a weak correlation between quality of chest compression perceived by each operator and its real effectiveness during cardiopulmonary resuscitation.
Keywords: Cardiopulmonary resuscitation, Cardiac arrest, Chest compression, Basic Life Support, Training
Background
In-hospital cardiac arrest, defined as sudden loss of cardiac function, is an event characterized by high morbidity and mortality [1–2]. As reported in literature its incidence is nearly 1–5 cases every 1000 hospitalized patients per year and the reported survival rate is nearly 15% at hospital discharge and 11% at 6 months [2–5]. Most of the survivors have good neurological outcome [3–5]. Until now a high-quality and uninterrupted chest compression is the cornerstone of cardiopulmonary resuscitation, increasing the chances of survival and improving the prognosis [6–7]. However, few studies considered the quality of chest compression even when it was performed by healthcare operators, reporting an average quality of this manoeuvre as sub-optimal [8–10]. Furthermore, several contrasting studies reported that some operator-depending variables were able to modify the quality of cardiopulmonary resuscitation in particular age, gender, weight, Body Mass Index (BMI), muscular fitness and hand applied to the thorax during cardiopulmonary resuscitation [10–17]. Aims of our study were to assess the quality of chest compression when it was performed by healthcare operator, to search any correlation between operator-related variables and effectiveness in performing cardiopulmonary resuscitation and to correlate self confidence with the maneuver and its real effectiveness.
Methods
In our prospective cohort study we enrolled a group of consecutive healthcare operators who were employed in a 500-bed second level Italian hospital (“Cardinal Massaia” Hospital in Asti, Italy) from February to October 2018.
Ethic
The investigation followed the principles outlined in the Declaration of Helsinki. We used a manikin for the study; therefore we did not consider any ethical approval. Any operator voluntarily accepted to take part at the research. All data used for the study were anonymously collected following national privacy law.
Protocol
Any healthcare worker performed a two-minute chest compression test on a high fidelity manikin (Laerdal Resuscitation Anne® Laerdal; Stawanger. Norway). The manikin stayed on the ground and the performance score was measured by the skill meter (Laerdal QCPR®, Laerdal; Stawanger Norway). This device was used in a “blind” modality (the operator could not see his own performance). It allowed assessing the quality of chest compression analyzing site of compression, its depth, frequency and release [7]. At the end of each performance the skill meter summarized the number of correct chest compression (correct hand position on chest, depth 5–6 cm, rate 100–120 compression per minute and complete release) over total number. This number, also known as compression score, ranged from 0% to 100% and showed in percentage the overall quality score of cardiopulmonary resuscitation practiced in time interval (2 minutes). It was considered adequate if ≥ 75% as described in a previous study [18].
End points
The primary end point was to record the quality of chest compression when it was performed by healthcare professional while secondary end points were to search variables related to high quality cardiopulmonary resuscitation and correlation between perceived quality of the manoeuvre and its real effectiveness.
Collected data
Age (years); weight (kilogram), height (meter), Body Mass Index (BMI) (Kg/m2), gender (male/female), smoke habit, hand applied on the thorax (dominant hand or not dominant hand), healthcare role (doctor/nurse/other), working area (medical/surgical/critical care/other), real life resuscitation experience and if referred physical limitation due to chronic low back pain or shoulder pain. Each operator at the end of performance reported his own self-confidence with the manoeuvre (bad/sufficient/good) and these data were subsequently compared with the real effectiveness recorded (compression score).
Statistic
Numerical variables were expressed as mean ± standard deviation (SD), while ordinal data as percentage. The relationship between quantitative variables (age and BMI) and compression score was valued using Pearson’s Linear Correlation Index. The qualitative variables were analyzed using the Shapiro-Wilk normalized ANOVA test. The homogeneity of variances between groups was verified with the Levene test. The Kruskal-Wallis test was performed to evaluate the difference between numerical data and the level of performance. The correlation between perceived quality of chest compression and its real effectiveness was analyzed with the Spearman Rank test.
Windows Excel Stat® program was used for statistical analysis.
P significant if < 0.05.
Results
We enrolled 60 consecutive healthcare operators. The average compression score realized during two minutes test was 70±19%. 48% of subjects reached a compression score adequate (≥75%), while in the other cases (52%) was below 75%. The performance quality is distributed as shown in figure 1.
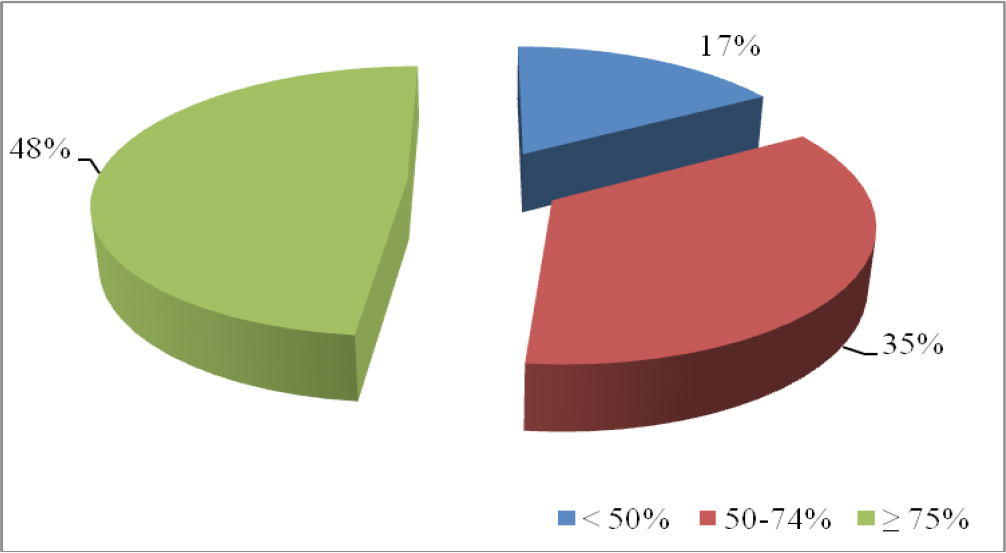
Figure 1: Distribution of the compression score (%).
Demographic and anthropometric data were: age 44±11 years, weight 68±11 Kg, height 1,67±0,07 cm and BMI 24±3 Kg/m2. These data did not correlate linearly with the quality of practiced chest compression during the test (r = 0.011). The other variables collected are summarized in table 1.
Table 1: Other operator-related variables.
|
Variable |
Percentage (%) |
Compression score (%) |
P |
|
Gender male female |
36.7 63.3 |
76±19 67±19 |
0.12 |
|
Smoke habit yes no |
30 70 |
76±19 68±19 |
0.18 |
|
Hand compressing thorax dominant not-dominant |
78.3 21.7 |
71±18 67±19 |
0.36 |
|
Healthcare role doctor nurse other |
18.3 63.3 18.3 |
74±19 72±19 65±13 |
0.27 |
|
Working area medical surgical critical other |
38.3 21.6 25 15 |
73±19 68±13 72±19 65±15 |
0.75 |
|
Real life resuscitation experience yes no |
58.5 41.7 |
75±19 65±19 |
0.04 |
|
Physical limitation yes no |
6.7 93.3 |
64±16 71±19 |
0.51 |
Among analyzed variables, the operators who previously performed a real-life cardiopulmonary resuscitation achieved a significantly higher level of compression score than those who had never practiced it on field (75±19% vs. 65±19%, p = 0.04) (Figure 2). After chest compression test over 90% of healthcare operators referred their manoeuvre as good or at least sufficient but in 51% of these tests the recorded compression score was below the adequate level of quality.
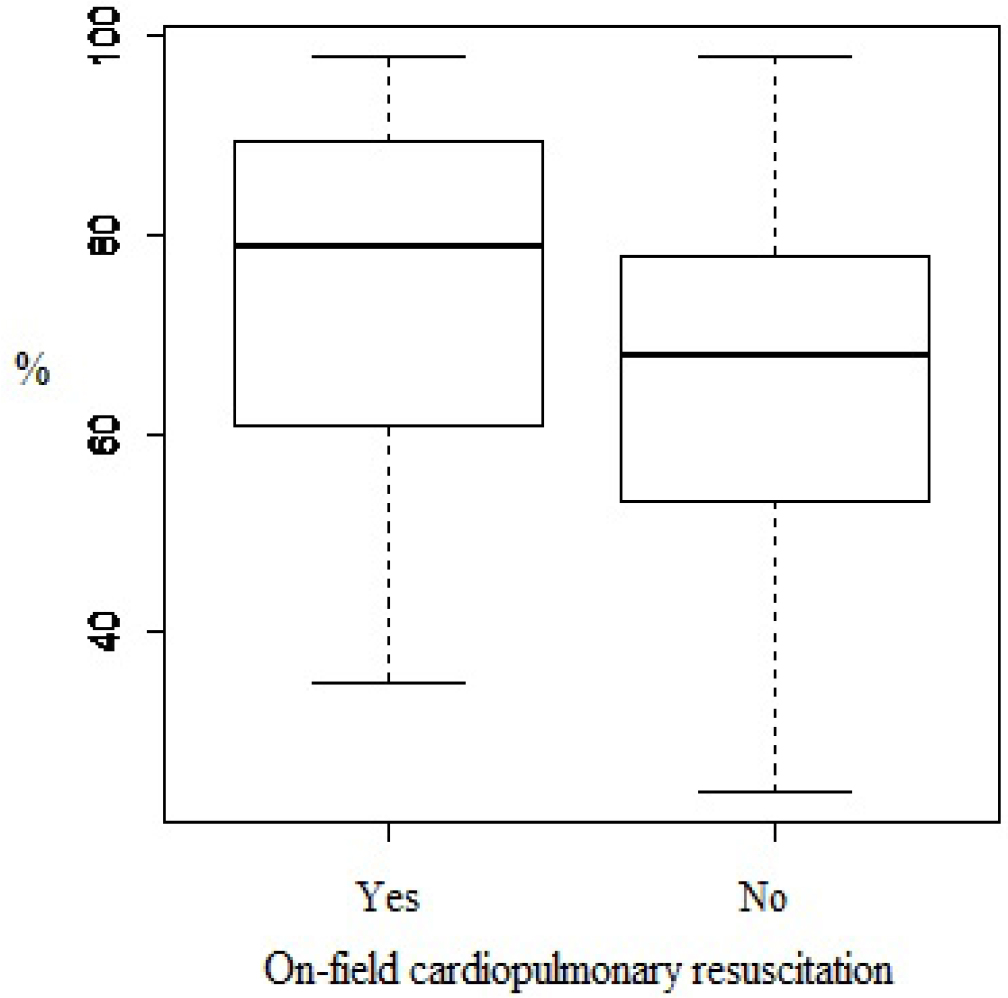
Figure 2: On field cardiopulmonary resuscitation experience and quality of chest compression (compression score in percentage) (p = 0.04)
Discussion
An uninterrupted and high quality chest compression is considered a cornerstone of the treatment during cardiopulmonary resuscitation [6–7]. Despite its main role during in hospital resuscitation, literature is scarce about quality of the procedure also if the manoeuvre is performed by healthcare operators. The main result from our study confirms that the quality of chest compression even if performed by healthcare operators is inadequate in nearly half of enrolled cases. In fact, 52% of healthcare operators realized a performance with a compression score below 75% confirming data from previous works. In a study realized using manikin, Pederby and collaborators concluded that chest compression was realized with a correct depth in only 46% of cases while in over 60% of tests the manoeuvre was practiced with a wrong frequency [10]. In another work the authors, analyzing data downloaded from defibrillator, found that in 37.4 % of cases chest compressions were incorrect for depth and in 40.9% for frequency.
Concerning operator-related variables, real life resuscitation experience was related to better chest compression. In fact we found that subjects who previously practiced a real cardiopulmonary resuscitation, practiced a better test than other healthcare operators without any previous experience (75±19% vs. 65±19%, p = 0.04). This result, recorded in our study, confirmed data shown in other work. In fact a previous study enrolling 296 nurses showed that on-field experience was related to better chest compression [19]. In our study no other variables were related to high quality of chest compression in contrast to other works. Peberdy et al. highlighted that increasing age made the quality of chest compression worse due to lower muscle mass and strength [10]. These data are different from our results where the group of subjects enrolled was homogenous by age. In our study gender did not correlate with the quality of chest compression contrasting with results derived from another work where the authors enrolled healthcare and novice operators showing a tendency of women to perform less efficient chest compression due to a higher frequency [17]. Furthermore Wang and coll. after a test lasting up to 8 minutes performed by military healthcare operators concluded that quality of chest compression could be related to gender, weight and BMI but only after the first two minutes of test [20]. The lack of correlation recorded in our study may be due to enrollment of only healthcare professionals and a relative shorter test according to the international guidelines (2 minutes).
Conflicting results are reported in literature about the effect of BMI on chest compression. The increasing BMI improved chest compression especially in cardiopulmonary resuscitation longer than 2 minutes [21]. On the other hand a value of BMI over 26 could modify negatively the manoeuvre due to a more incomplete chest release at the end of the massage and an abnormal body position due to the weight itself [17]. Concerning the hand applied on the thorax and used during chest compression no difference were seen in our work despite positive results in other studies where practiced chest compression was better using dominant hand during a cardiopulmonary resuscitation longer than 2 minutes and when performed by novice rescuers [12,22].
In the end, in our work we showed that real quality of chest compression was not related to its perception during the maneuver. In fact, in 51% of those who considered their test as sufficient or good the real quality was suboptimal. The same rate of incorrect perception of maneuver’s efficacy was seen in a multicenter study where real and perceived quality in cardiopulmonary resuscitation did not correlate in over 60% of subjects [14]. These data support the need of a device able to show the quality of manoeuvre during cardiopulmonary resuscitation.
The main limit of the study is linked to the sample size. This could explain the lack of significant difference in some subgroups of operators different for working area and role. In addition, data obtained from a training test should be cautiously generalized in clinical practice. In fact, the study realized using manikin is more feasible and easier, avoiding direct involvement of healthcare operator but the results must be contextualized to the reality in which the test took place. The “experimental” environment is very different from clinical practice. In particular, real cardiopulmonary resuscitation is burdened by emotional share that could impact on the quality of the manoeuvre.
In conclusion, the quality of chest compression is an ever improving and testing topic in resuscitation therapy even when performed by healthcare operators where achieved satisfactory efficacy in nearly half of cases analyzed. Among quality related variables real life previous resuscitation experience was connected to better performance rather than other variables.
In the end, we may reinforce the need to use a feedback device able to provide feedback about adequacy of performed chest compression.
Acknowledgement
The principal investigator, Roasio Agostino and Giorgio Bergesio, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
References
- Priori SG, Aliot E, Blomstrom-Lundqvist C, Bossaert L, Breithardt G, Brugada P, et al. (2002) Task force on sudden cardiac death, European society of cardiology. Europace 4: 3–18. [View]
- Sandroni C, Nolan J, Cavallaro F, Antonelli M (2007) In hospital cardiac arrest: incidence, prognosis and possible measures to improve survival. Intensive Care Med 33: 237–245. [View]
- Nolan JP, Soar J, Smith GB, Gwinnut C, Parrott F, Power S, et al. (2014) Incidence and outcome of in-hospital cardiac arrest in the United Kingdom National Cardiac Arrest Audit. Resuscitation 85: 987–992. [View]
- Radeschi G, Mina A, Berta G, Fassiola A, Roasio A, Urso F, et al. (2017) Incidence and outcome of in-hospital cardiac arrest in Italy: a multicentre observational study in the Piedmont Region. Resuscitation 119: 48–55. [View]
- Andersen LW, Holmberg MJ, Lofgren B, Kirkegaard H, Granfeldt A (2019) Adult in-hospital cardiac arrest in Denmark. Resuscitation 140: 31–36. [View]
- Travers AH, Perkins GD, Berg RA, Castren M, Considine J, Escalante R, et al. (2015) Part 3: Adult Basic Life Support and Automated External Defibrillation: 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation 20:132:S51–83. [View]
- Perkins G, Olasveengen TM, Maconochie I, Soar J, Willie J, Greif R, al. (2018) European Resuscitation Council Guidelines for Resuscitation: 2017 update. Resuscitation 123: 43–50. [View]
- Abella BS, Alvarado JP, Myklebust H, Edelson DP, Barry A, O’Hearn N, et al. (2005) Quality of Cardiopulmonary Resuscitation During In-Hospital Cardiac Arrest. JAMA 293: 305–310. [View]
- Semark B, Årestedt K, Israelsson J, von Wangenheim B, Carlsson J, Schildmeijer K (2017) Quality of chest compressions by healthcare professionals using real-time audiovisual feedback during in-hospital cardiopulmonary resuscitation. Eur J Cardiovasc Nurs. 16: 453–457. [View]
- Peberdy M.A, Silver A, Ornato JP (2009) Effect of caregiver gender, age, and feedback prompts on chest compression rate and depth. Resuscitation 80: 1169–1174. [View]
- Körber MI, Köhler T, Weiss V, Pfister R, Michels G (2016) Quality of Basic Life Support – A Comparison between Medical Students and Paramedics. J Clin Diagn Res 10: OC33-OC37. [View]
- Wang J, Tang C, Zhang L, Gong Y, Yin C, Li Y. (2015) Compressing with dominant hand improves quality of manual chest compressions for rescuers who performed suboptimal CPR in manikins. Am J Emerg Med 33: 931–36. [View]
- Ashton A, McCluskey A, Gwinnutt CL, Keenan AM (2002) Effect of rescuer fatigue on performance of continuous external chest compressions over 3 min. Resuscitation 55: 151–5. [View]
- Cheng A, Overly F, Kessler D, Nadkami VM, Lin Y, Doan Q, et al. (2015) Perception of CPR quality: Influence of CPR feedback, Just-in-Time CPR training and provider role. Resuscitation 2015;87:44–50. [View]
- Yang Z, Li H, Yu T, Chen C, Xu J, Chu Y, et al. (2014) Quality of chest compressions during compression-only CPR: a comparative analysis following the 2005 and 2010 American Heart Association guidelines. Am J Emerg Med 32: 50–54. [View]
- López-González A, Sánchez-López M, Garcia-Hermoso A, Lopez-Tendero J, Rabanales-Sotos J, Martinez-Vizcaino V (2016) Muscular fitness as a mediator of quality cardiopulmonary resuscitation. Am J Emerg Med 34: 1845–1849. [View]
- Jaafar A, Abdulwahab M, Al-Hashemi E (2015) Influence of Rescuers’ Gender and Body Mass Index on Cardiopulmonary Resuscitation according to the American Heart Association. 2010 Resuscitation Guidelines. Int Sch Res Notices 246398. [View]
- Cortegiani A, Russotto V, Montalto F, Iozzo P, Meschis R, Pugliesi M, et al. (2017) Use of Real-Time Training Software (Laerdal QCPR®) Compared to Instructor-Based Feedback for High-Quality Chest Compressions Acquisition in Secondary School Students: A Randomized Trial. Plos ONE 12: e0169591. [View]
- Verplancke T, De Paepe P, Calle PA, De Regge M, Van Maele G, Monsieurs KG (2008) Determinants of the quality of basic life support by hospital nurses. Resuscitation 77: 75—80. [View]
- Wang J, Zhuo CN, Zhang L, Gong YS, Yin CL, Li YQ (2015) Performance of cardiopulmonary resuscitation during prolonged basic life support in military medical university students: A manikin study. World J Emerg Med 6: 179–85. [View]
- Wang J, Zhuo CN, Zhang L, Gong YS, Yin CL, Li YQ (2015) Performance of cardiopulmonary resuscitation during prolonged basic life support in military medical university students: A manikin study. World J Emerg Med 6: 179–85. [View]
- You Js, Kim H, Park JS, Baek KM, Jang MS, Lee HS, Chung SP, Kim SW (2015) Relative effectiveness of dominant versus non-dominant hand position for rescuer’s side of approach during chest compressions between right-handed and left-handed novice rescuers. Emerg Med J 32: 184–8. [View]